
One more benefit of visiting the store is to get the Foot Analsysis.

You’ve shared your ASICS Foot ID scan (01-Mar-2026). I’ll interpret it clinically and translate that into marathon-specific training adjustments.
1️⃣ Key Structural Findings from Your Scan
📏 Size & Width
Size: 27 (JP) both feet (~US 9)
Width: 2E (wide) both feet
→ You need wide-platform shoes (important for stability + toe splay).
2️⃣ Forefoot & Toe Alignment



Toe angle: Mild valgus tendency (especially right ~7.3°)
Slight asymmetry between L and R
Ball girth: Medium-to-wide
What This Means
Mild tendency toward hallux valgus mechanics
You need:
Wide toe box
Strong intrinsic foot muscles
Avoid narrow racing shoes
3️⃣ Heel Alignment & Rearfoot Control



Heel angle: Slight valgus tendency
Heel breadth: Moderate
Pressure pattern shows heel + forefoot loading
Interpretation
You likely:
Mild pronation during stance
Load heel first, then push through forefoot
Not severe overpronator — but not neutral either
For marathon → you need controlled stability, not motion control.
4️⃣ Arch Height & Instep


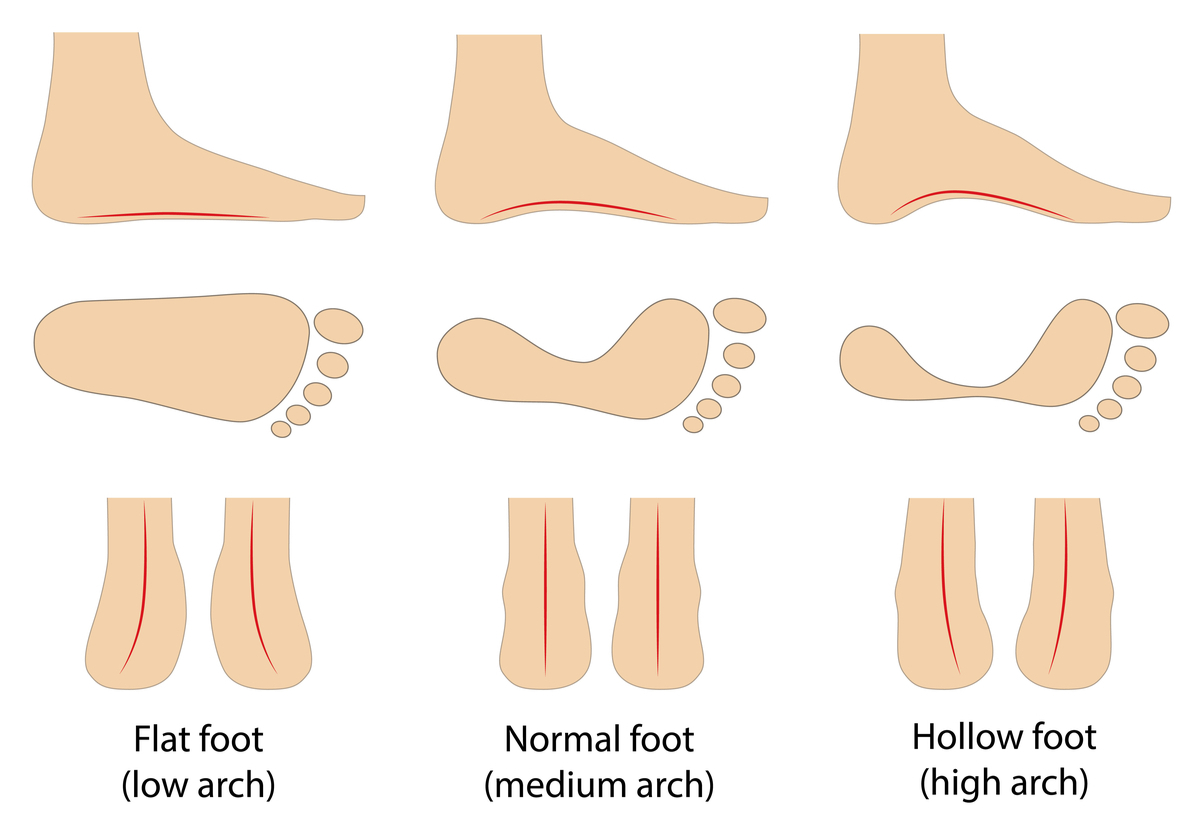

Arch height: Medium (slightly toward high on right)
Instep height: Moderate-high
Pressure map shows decent midfoot contact
Meaning
You are not flat-footed.
You don’t need heavy orthotics unless symptomatic.
🔬 Biomechanical Summary
You are:
✔ Wide foot (2E)
✔ Mild valgus toe
✔ Mild rearfoot valgus
✔ Medium arch
✔ Slight L/R asymmetry
Profile = Mild pronation + wide forefoot + stable arch
This is manageable with proper strength work.
🏃 Marathon Training Adjustments (Important)
Given your running history (you’re already clocking 8–9 km runs at ~6:26/km with HR ~154 bpm), here’s how you should train:
1️⃣ Shoe Strategy (Critical)
Use:
Stability shoe (mild guidance)
Wide (2E)
Firm midsole
Avoid:
Narrow carbon racers for long runs
Soft unstable trainers
2️⃣ Strength Protocol (Mandatory for You)
Do this 3x/week:
A. Foot Intrinsics (10 min)
Short foot exercise
Toe yoga
Towel scrunch
Barefoot balance holds
B. Posterior Chain (Essential)
Because mild valgus = hip weakness link.
Single leg RDL – 3×10
Bulgarian split squats – 3×8
Side plank with leg lift – 3×30s
Clamshells – 3×15
3️⃣ Running Form Focus
You must:
Increase cadence to 170–178
Avoid overstriding
Slight forward lean from ankles
Keep knee tracking straight (avoid collapse inward)
4️⃣ Long Run Structure (For You Specifically)
Because of mild pronation:
✔ Increase mileage gradually (no >10% jump)
✔ Keep long runs conversational pace
✔ Avoid excessive cambered roads
✔ Do strides (6×100m) after easy runs
5️⃣ Injury Watch List (Based on Scan)
You’re slightly prone to:
Plantar fasciitis
Tibialis posterior strain
IT band tightness (due to valgus chain)
Preventive:
Calf raises (bent + straight knee)
Tibialis posterior strengthening (band inversion)
Foam roll lateral quad
📊 How You Should Progress Toward Marathon
If targeting sub-4:30 marathon:
Phase structure:
Base Phase (8–10 weeks)
4 runs/week
30–45 km/week
1 tempo
1 long run
Build Phase
Add intervals
Long runs up to 30–32 km
Peak Phase
Marathon pace segments inside long run
🎯 Most Important for YOU
Your scan does NOT show a severe structural issue.
Your limiter will NOT be foot mechanics.
It will be:
Aerobic base
Muscular endurance
Body weight management (if applicable)
Consistency
No comments:
Post a Comment